
The Hospital Cash Printer
Part 2 of our drug pricing posts - covering the 340B program

In our last post we covered the basics of drug pricing and focused on PBMs. Mainly how they dictate how much pharmacies and patients spend on drugs.
Today we’re going to cover another part of drug pricing. Specifically how hospitals and large-chain pharmacies are pocketing billions of dollars by exploiting a government program.
Today’s post will be more of a fact sheet as opposed to a meme-filled exposé like the PBM piece. Believe us, we tried w/ the memes on this one, but turns out drug pricing programs are quite unmemeable.
And on the surface the program seems nothing like a cash printer - in fact it’s quite the opposite!
It’s a drug discount program called 340B, created to help hospitals serve under-insured and poorer patients.
But like most stuff in healthcare, there’s more than meets the eye.
The basics about 340B
340B is a federal initiative that requires drug manufacturers (who participate in Medicaid) to provide outpatient drugs to eligible healthcare organizations, known as "covered entities," at significantly reduced prices.
These discounts typically range from 20% to 50% off the drug's list price, and are given with the intent to "stretch scarce federal resources as far as possible, reaching more eligible patients and providing more comprehensive services."
Covered entities are providers serving high volumes of uninsured and low-income patients such as:
Children's Hospitals
Pivotal moments in the 340B timeline are:
1992 - The 340B program was established by Congress as part of the Veterans Health Care Act of 1992. It was a response to concerns that the Medicaid drug rebate program, enacted two years earlier, might lead to increased drug prices for safety-net providers.
1996 - Initially, covered entities could only use in-house pharmacies to dispense 340B drugs. Recognizing that many entities lacked such facilities, the Health Resources and Services Administration (HRSA) allowed them to contract with a single outside pharmacy.
2010 - The ACA significantly expanded 340B in several ways.
Added more types of hospitals to the list of eligible entities, including critical access hospitals, sole community hospitals, rural referral centers, and free-standing cancer hospitals.
Allowed covered entities to contract with multiple pharmacies, leading to explosive growth in contract pharmacy arrangements.
Contract pharmacies are retail pharmacies that partner with covered entities to dispense 340B drugs.
And 340B has had positive impact in terms of delivering care:
Critical Access Hospitals: 75% report that 340B savings help them remain open.
Federally Qualified Health Centers: Many use 340B savings to provide care to more patients or offer more comprehensive services.
Ryan White Clinics: These facilities, which provide care for half of the population with HIV/AIDS in the U.S., use 340B savings to offer free or low-cost care and support services like housing and food assistance.
Some hospitals and clinics are able to stay solvent exclusively due to 340B, which is huge for health accessibility. However, the growth of 340B has led to some unintended consequences.
Show me the money!
340B has seen dramatic growth since it’s inception:
In 2000, there were just over 8,100 covered entity sites.
By 2020, this number had grown to 50,000.
Hospitals, which initially made up less than 10% of covered entity sites, comprised over 60% by 2020.
Total 340B drug purchases have skyrocketed from about $4 billion in 2007-2009 to $53 billion in 2022.
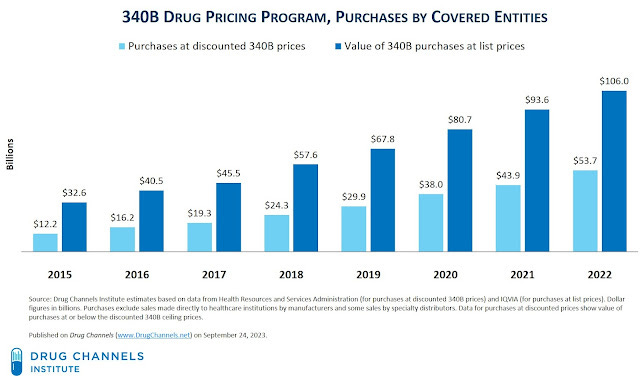
This should mean that in 2022 there were $50B+ saved in drug costs for this population, but here’s the kicker - hospitals don’t have to report the rebates or how they’re used.
So no one actually knows whether that money is being used for uninsured/lower-income populations.
And because they don’t have to report the rebate, the insurance company has no clue about it. Allowing hospitals to submit the wholesale price for insurance reimbursement!

Additionally contract pharmacies have also exploded which should mean that there’s an increase of access to the drugs for low-income/uninsured populations.
However, it turns out as of 2022, an astonishing 71% of locations among the top four retail pharmacy chains (Walmart, CVS, Rite Aid, and Walgreens) held 340B contracts. And they too make a profit margin based on higher reimbursement rates from insurance companies - with Walgreens even warning of lower profits due to impending 340B restrictions.
So this discount program has now become a source of profits. Many such cases in American healthcare.
Current Challenges and Debates
The 340B program is currently at the center of various legal and policy debates, including legislative attempts to modify the program, legal battles between stakeholders, and calls for reform to increase transparency and oversight.
Here’s a broad overview of the types of solutions that are at play:
Legislative Attempts: Multiple bills have been introduced in Congress to modify the program, focusing on issues like tightening eligibility criteria, increasing transparency, and regulating contract pharmacy arrangements.
Legal Battles: Recent years have seen numerous lawsuits between drug manufacturers, covered entities, and the government. Key issues include manufacturers' attempts to limit 340B pricing for drugs dispensed at contract pharmacies and disputes over the calculation of 340B ceiling prices.
Calls for Reform: Various stakeholders are pushing for changes to the program, including: Increased transparency in how 340B savings are used More stringent eligibility requirements for hospitals Clearer definition of eligible patients Greater oversight of contract pharmacy arrangements
Regulatory Challenges: The Health Resources and Services Administration (HRSA), which oversees 340B, faces challenges in effectively regulating the program due to limited statutory authority.
All in all our takeaway is that this is mainly a regulatory issue in healthcare.
We’re interested in seeing if tools helping track rebates and drug purchasing data can be a tech-forward solution in combatting 340B misuse, but it’s highly unlikely to be effective unless there are compliance requirements by law.
So for now, we’ll just have to wait and see if policy is introduced to combat the misuse of 340B.
If you’ve made it this far, we hope you now are better informed about how even drug discounts can be money-makers!
We’re always looking to learn from others, so if you have any thoughts or building something in this space please feel free to reach out.
And if there’s anything you were curious about or think we should modify/add let us know!